
From the 1Hacettepe University Medical School, Department of Physical and Rehabilitation Medicine, Ankara, Turkey and 2IRCCS Rizzoli Orthopaedic Institute, Department of Biomedical and Neuromotor Science, Physical and Rehabilitation Medicine Unit, Bologna, Italy.
E-mail: vincenzo.ricci58@gmail.com
Accepted Jan 30, 2019; Epub ahead of print Feb 15, 2019
Interest in ultrasound (US) imaging and its utility in clinical practice among Physical and Rehabilitation Medicine (PRM) physicians is ever-increasing (1, 2). Similar to the development of new diagnostic and therapeutic skills, the use of US imaging provides a “new language” for our specialty.
Anatomically, we can now directly visualize different compartments and tissues of the musculoskeletal system. In contrast to classical knowledge, this provides better understanding of the condition of our patients (3). Now, the shape, thickness, length, and reciprocal relationships among nearby structures (which differ from person to person) are no longer the result of memory, but are a simple observation of the biological system. “Seeing is believing”, and factors that can be visualized can also be (semi)quantified (Fig. 1A) (4, 5).
In addition, visualization can be used for exploration of particular structures/pathologies in cases where surgery cannot be performed. For instance, an aberrant vessel inside an otherwise healthy nerve cannot be seen during surgery unless resection is performed. However, with US imaging this can conveniently and comparatively be done without harm to the patient (6). As such, we have started to talk about “virtual dissection”.
Secondly, real-time dynamic scanning provides a superior approach during patient examination. Observing the normal and pathological movements of a muscle, joint or tendon helps to integrate the complex knowledge of biomechanical analysis with the clinical complaints (Video 11). A muscle herniating during contraction, a tendon/ligament being partially detached while moving, or a calcification impeding the joint motion, would definitely be explanatory enough when coupled with the onset of painful symptoms during assessment (Video 21) (7). At this stage, probe compression can also be used to precisely localize the pathology. Therefore, considering the fact that the US probe has become the “stethoscope”’ or the “sixth finger” of a physiatrist, we also speak about “sono-auscultation”’ or “sono-palpation”, “sono-Tinel” and “self-palpation” (Fig. 1B & C) (8).
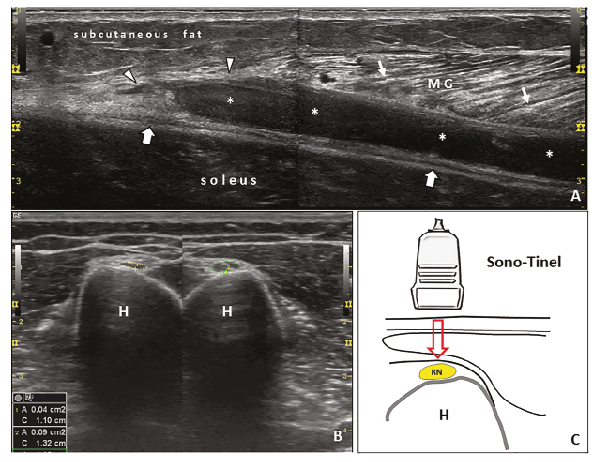
Fig. 1. (A) “Seeing the pathology after history-taking and physical examination”. Split-screen panoramic imaging of the calf shows a strain lesion at the myotendinous junction (arrowheads) of the medial head of the gastrocnemius muscle (GM); “tennis leg”. A widespread haematoma (asterisks) is seen between the layers of the intermuscular fascia (thick arrows). Note that the muscle fibres are relatively spread, i.e. with normal pennate architecture (thin arrows). (B) “Sono-palpation” and (C) “Sono-Tinel”. Using the probe for palpating on/nearby the painful area indisputably helps the physician “complete” the physical examination and provides further insight as regards the underlying problem. Yet, a positive “sono-palpation”, coupled with the presence of an abnormal ultrasonographic finding, is invaluable for precise diagnosis. In this comparative short-axis imaging (B), radial nerve cross-sectional area measurements are seen in exactly the area the patient described a positive “sono-Tinel” (C), i.e. pain or dysaesthesia on probe compression. The nerve is significantly swollen at the spiral groove level and the clinical diagnosis of “Saturday night palsy” is promptly confirmed. MG: medial gastrocnemius; H: humerus; RN: radial nerve.
Thirdly, the other useful philosophy pertaining to the utility of US in PRM is that once one is able to visualize a structure/pathology one can readily target it. Thus, the use of US-guidance for interventional physiatry has been increasing rapidly, and this issue also necessitates further terminologies (9). For instance, we are no longer discussing ordinary interventions, such as “shoulder injection” or “carpal tunnel injection”. In light of the initial US imaging (findings), we need to specify the details of the procedure; thus, we have started to use more descriptive wording, such as like “intralesional platelet-rich plasma injection for a bursal-side partial thickness incomplete tear of the supraspinatus tendon” or “’hydrodissection of the median nerve from the flexor retinaculum using the ulnar-side in-plane approach”, respectively (Video 31). In short, for US-guided interventions, we need to clarify the exact lesion, the precise target and the prompt injectate and technique (10). This raises the question of whether we will still use the same (or a new) language after US has been widely welcomed into PRM.


 Click to show fullsize
Click to show fullsize